Cerebellar Dysfunctions Associated with a Developmental Venous Anomaly
Article information

Abstract
A developmental venous anomaly (DVA) is a congenital vascular malformation characterized by dilated medullary veins. In the majority of cases, a DVA is asymptomatic and typically, incidentally diagnosed on magnetic resonance imaging and angiography. However, when a DVA is located in the cerebellum, patients may experience symptoms such as hearing disturbance, tinnitus, and dizziness, which are often attributed to mechanical or flow-related issues. In this report, we present the case of a 70-year-old patient who complained of dizziness, along with cerebellar dysfunctions, due to a DVA.
A developmental venous anomaly (DVA) is a type of vascular malformation characterized by a mass-like lesion consisting of dilated medullary veins. Its incidence rate ranges from 0.48% to 2.56%.1 Typically, DVAs remain asymptomatic or are incidentally discovered during imaging studies. Brain magnetic resonance imaging (MRI) reveals a distinctive “caput medusae” appearance or an umbrella-like structure formed by the convergence of small cerebral veins, which then merge into one or two draining veins.2 When a DVA is located in the cerebellum, patients may experience symptoms such as hearing disturbances, tinnitus, and dizziness due to seizures, intracranial hemorrhage, and ischemic stroke.3,4 In this report, we present a case with an 8-month history of dizziness and progressively worsening cerebellar dysfunctions attributed to an extensive bilateral cerebellar DVA.
CASE
A 70-year-old male was admitted to the hospital due to persistent dizziness and cerebellar dysfunction lasting for eight months. He had no prior history of medication or disease. The dizziness was described as non-rotational, persisting even at rest and exacerbated with movement. Additional symptoms such as nausea, vomiting, ataxia, hearing loss, tinnitus, and headaches were notably absent. Upon neurological examination, dysarthria and a wide-based gait with instability during straight-line walking were observed. Video oculography and nystagmography examinations revealed spontaneous nystagmus to the left when his head was kept still, and an upward drift followed by downbeat nystagmus during the upward movement in primary gaze was observed (Fig. 1). The video head impulse test indicated a reduced upward gain compared to a downward gain in the vertical optokinetic saccades. Extensive blood tests, general chemistry panels, and neoplastic/paraneoplastic disease screenings showed no abnormalities. Autonomic nervous system tests and [123I] N-omega-fluoropropyl-2beta-carbomethoxy-3beta-{4-iodophenyl} nortropane ([123I] FP-CIT) scans also failed to reveal any abnormalities that could explain the patient’s symptoms.
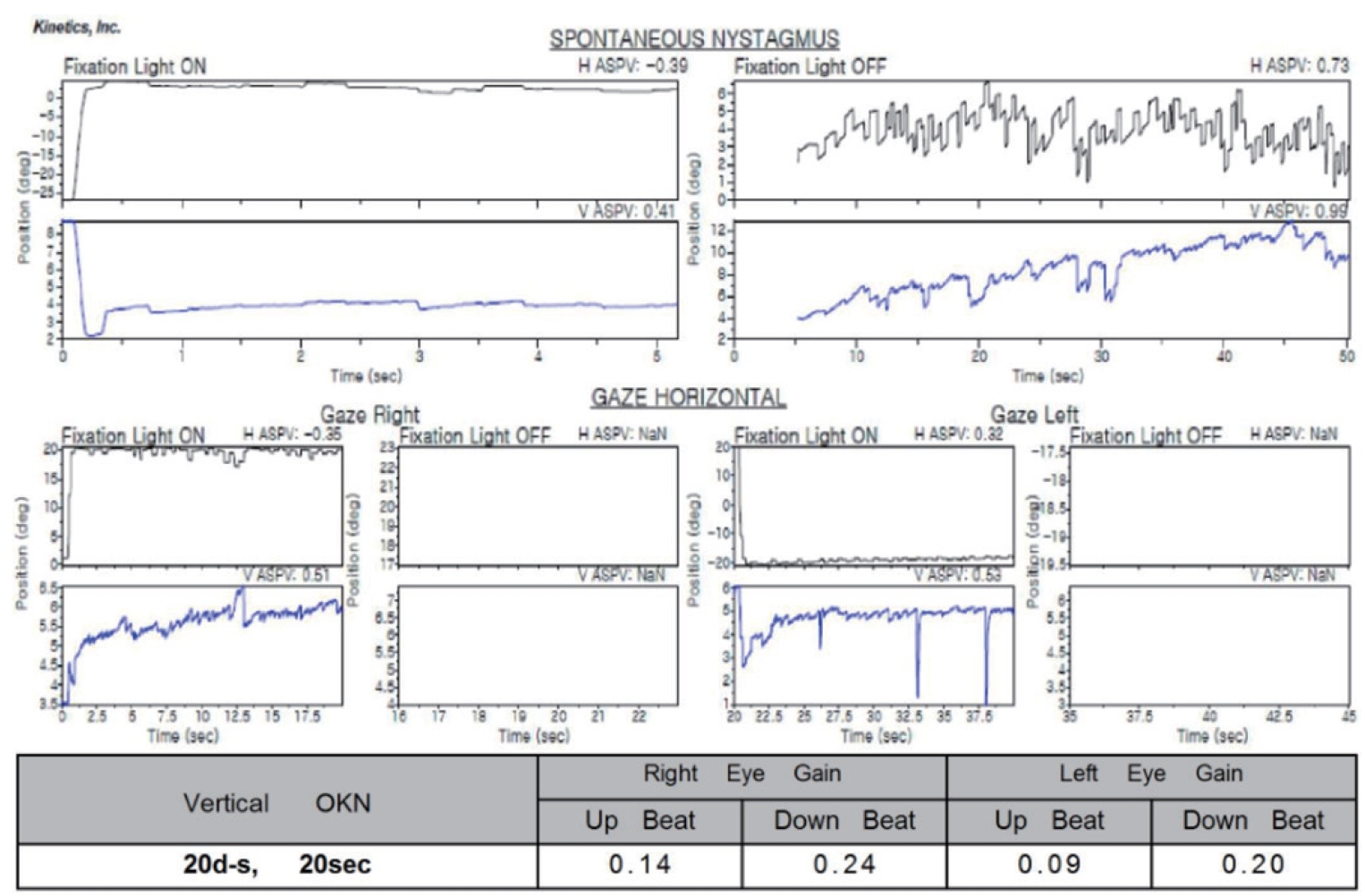
Video oculography and video nystagmography; leftward spontaneous nystagmus at rest, with an upward drift transitioning into downbeat nystagmus during upward gaze in the primary position.
MRI scans revealed intensified bilateral cerebellar venous malformations extending from the tonsil to the hemispheres on contrast-enhanced T1-weighted and susceptibility-weighted images and confirmed the absence of other vascular structural abnormalities (such as cavernous malformation or dural arteriovenous fistula). Digital subtraction angiography confirmed the venous structure, with a draining vein leading from the left hemisphere to the cerebellar vermis, connected to the vein of Galen. A mild stenosis at the venous collector was observed (Fig. 2). The patient received conservative treatment with ginkgo biloba. Subsequently, the patient was discharged and is currently undergoing regular follow-up observation.
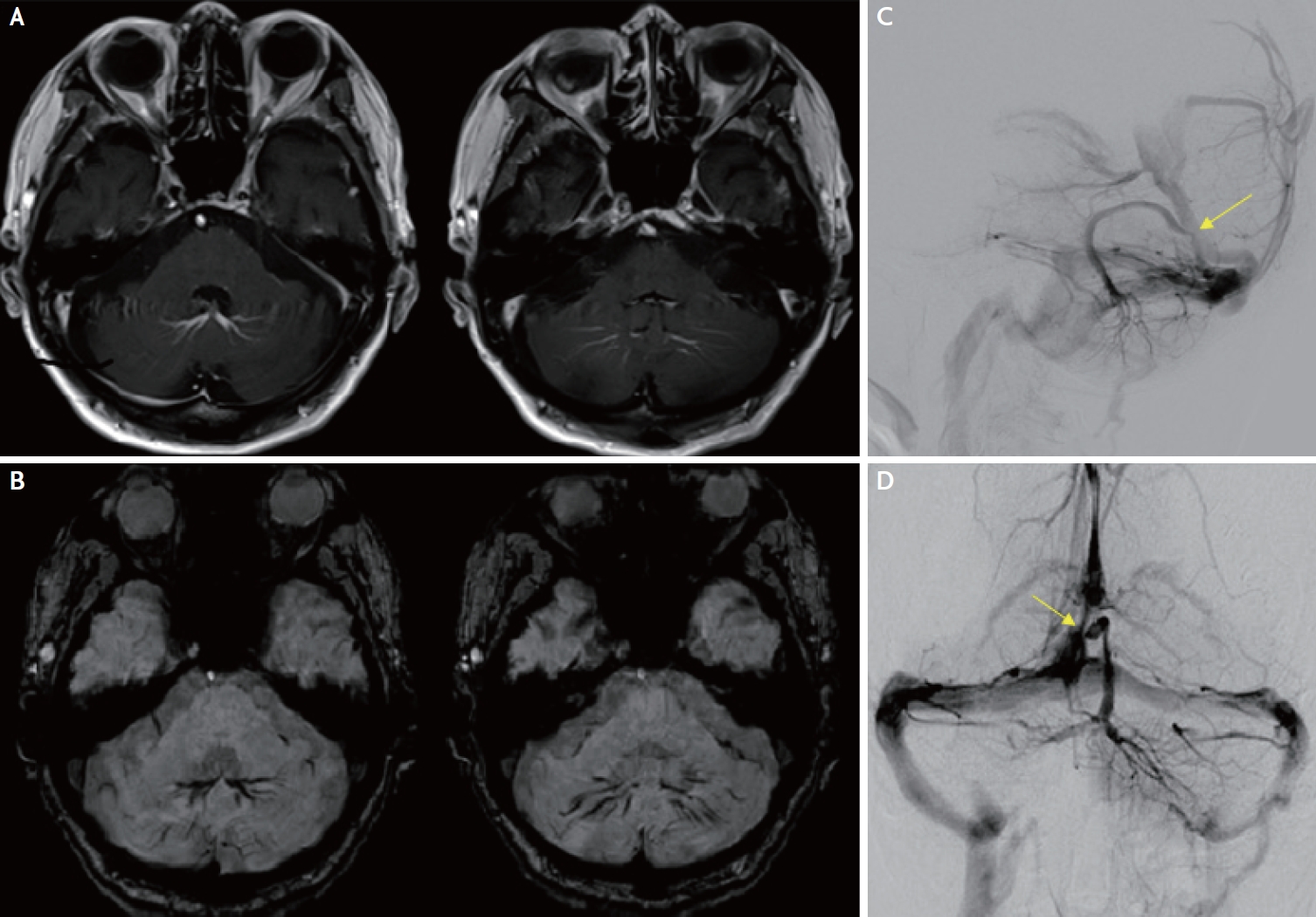
(A) Contrast-enhanced T1-weighted sequence showing developmental venous anomalies in both cerebella adjacent to the vermis. (B) Susceptibility weighted image. (C) Sagittal view of the digital subtraction angiography image. (D) Coronal view of the digital subtraction angiography image. Arrowhead shows mild stenosis at the venous collector.
DISCUSSION
This case involved a 70-year-old male patient who experienced prolonged dizziness and cerebellar dysfunction over an 8-month period, which was indicative of a cerebellar DVA. Neuro-ophthalmologic findings strongly suggested a central cause for the patient’s signs and symptoms. Since the patient did not exhibit additional features associated with degenerative diseases or autonomic dysfunction and considering the relatively rapid progression of clinical symptoms in conjunction with the presence of a cerebellar DVA, it was concluded that the symptoms were primarily attributable to the cerebellar DVA.
A DVA is commonly found at the frontal and parietal lobes, although approximately 14–27% of cases manifest in the cerebellum.5 Clinical presentations of DVAs can vary widely, encompassing asymptomatic cases, as well as symptomatic ones characterized by symptoms such as nausea, vomiting, dizziness, nystagmus, and headaches.6 The mechanisms contributing to symptomatic cerebellar DVAs include the compression of adjacent brain structures and hemodynamic changes stemming from increased blood inflow (micro shunts to DVAs or arteriovenous malformation draining into the DVA) or decreased outflow (obstruction of the venous collector or draining sinus or presence of a distant high flow shunt).5 Moreover, reduced outflow can lead to congestion, potentially resulting in thrombosis or occlusion.5 It is worth noting that infratentorial lesions are often accompanied by cavernous malformation, which increases the risk of bleeding when compared to supratentorial lesions.7
In this patient, there was mild stenosis at the venous collector, but without a venous infarction or hemorrhage. The brain MRI and angiography results clearly showed venous structures extending from the cerebellar tonsils to the uvula, forming collecting veins. These findings were most pronounced in the parenchyma adjacent to the cerebellar nodulus. Therefore, it is reasonable to consider that the patient’s cerebellar dysfunction symptoms may be attributed to the mechanical compression resulting from the cerebellar DVA itself.8
A DVA is typically diagnosed using MRI, while angiography is valuable for assessing the hemodynamics, potential rupture risks, presence of stenosis, arteriovenous malformations, and other structural details.9 Although there is no standardized treatment for DVAs, conservative medication is generally recommended for asymptomatic or mildly symptomatic cases.4 Anticoagulation therapy may be considered for cases involving concomitant ischemia or venous thrombosis, and shunting or surgical intervention might be options for cases associated with hydrocephalus.9 In this particular case, despite undergoing conservative treatment, the patient’s symptoms did not show a significant improvement. Therefore, it is advisable to conduct serial follow-up examinations to monitor the progression of the DVA and the potential development of any complications. Perfusion imaging could also be beneficial in understanding how the venous angioma affects symptom changes based on alterations in hemodynamic state.
To date, there have been no reports of patients with complaints of cerebellar dysfunctions due to cerebellar DVAs with mechanical compression regardless of parenchymal lesions. Further research and advancements in imaging techniques are vital to better diagnose and treat individuals affected by this intriguing vascular anomaly.
Notes
Ethics Statement
Informed consent for publication was obtained from the patient.
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author upon reasonable request.
Sources of Funding
None.
Conflicts of Interest
No potential conflicts of interest relevant to this article was reported.
Acknowledgements
None.